对于任何肺活检来说,处理呼吸运动都是一个困难的挑战,尤其是对于不在肺尖部或肺上段的小结节。运动的程度取决于目标的位置 (在横膈膜附近最大) 和慢性阻塞性肺疾病和肥胖等患者因素。第一步是适度镇静,以实现稳定的浅呼吸。通过小剂量的反复给药来维持稳定的镇静水平是促进精确靶向的关键。另一个技巧是在呼吸周期的同一点成像和推进针,理想的是在全麻下呼吸暂停。
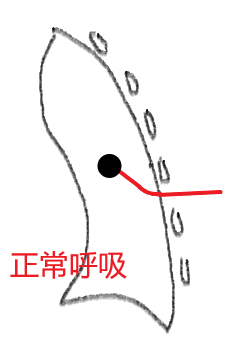
Respiratory volume should remain within the range of normal, quiet breathing.
呼吸容量应保持在正常、平静的呼吸的范围内。
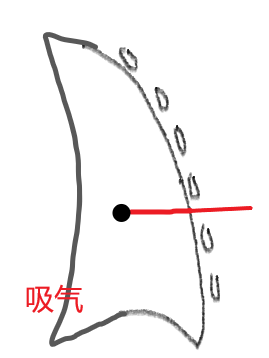
A puncture during a deep inspiration or expiration results in tension on the needle when the lung returns to its more normal status.
在深吸气或呼气时,当肺恢复到正常状态时,穿刺会导致针的紧张力。
This theoretically places greater stress on the pleura at the puncture site increasing the likelihood of a pleural tear.
理论上,这对穿刺部位的胸膜造成更大的压力,增加了胸膜撕裂的可能性。
During sampling, care should be made not to create tension on the needle; ideally, the patient holds his/her breath while the radiologist is sampling.
在取样时,应注意不要对针造成张力;理想情况下,病人在放射科医生取样时屏住呼吸。
Patients are better able to hold a breath in inspiration than in expiration.
病人在吸气时比在呼气时更能屏住呼吸。
Once a person can no longer hold breath, the tendency is to exhale if an inspiration was held but to inhale if an expiration was held.
一旦患者不能再屏住呼吸,如果吸气就呼气,如果保持呼气就吸气。
呼气末屏住呼吸活检 Bx in end-expiratory breathhold
The latter is more likely to cause an air embolism.
|