结直肠癌(CRC)是癌症相关死亡的主要原因【1】。在欧洲2006年,有412,900的原发性结直肠癌确诊新病例,其中207,500人死亡【2】。肝脏是结直肠癌最常见的转移脏器部位(MCRC)。因此肝转移是结直肠癌患者的复发和死亡的主要原因【3】。大约15–25%诊断为结直肠癌患者同时有肝转移,而另外15–20%的病人原发灶切除后3年内会出现异时性肝转移【4】。如果不治疗,转移性结直肠癌患者的中位生存期是6-8个月【5】)。由于肝脏病变的位置、大小或数量,不到25%的患者的肝转移是手术治疗的适应症【6】。然而,有或无围手术期化疗,3年内65–72%的病人会出现肝转移病灶切除术后肝内复发 【7】.。
对于不能手术切除的大多数患者,现代化疗方案联合靶向药物的使用大大延长中位生存时间为24个月【8,9】。然而,转移性结直肠癌患者多数患者会进展除非手术切除。对于常规化疗方案失败的结直肠癌肝转移患者,仍需进行有效的治疗。
放疗栓塞疗法针对不能手术的原发或继发性肝脏肿瘤提供有针对性的放射治疗。这种近距离的放射治疗可能与化疗同时使用,较单用化疗提高治疗反应和延长疾病进展时间和生存期【10,11】,或作为单药治疗或化疗治疗中断期间或难治性化疗患者,它是一种新兴的、重要的和有效的治疗选择【12,13】。
放疗栓塞疗法所用90钇(90Y)是一种永久地绑定到有较好生物相容性的非生物降解微球,玻璃或树脂制作。它是是一种纯β发射器衰减到稳定的锆(zirconium-9)平均能量为0.94(MeV)兆电子伏和半衰期为2.67 days (64.2小时).。钇90的1GBq(gigabecquere,千兆贝克勒尔)约27mCi释放较高(总剂量50Gy kg−1),但局限的β射线,平均组织穿透2.5mm,最大范围11mm 【14】。钇90通过经皮股动脉穿刺导管释放到肝动脉内,通过其分支优先进入肝转移病灶的新生血管内,并释放肿瘤杀伤(tumouricidal)的辐射剂量。
如果不考虑医学经济因素,我们追求一项肿瘤治疗或联合治疗的疗效时,最终目标是它的整体生存率(overall survive)。但由于医学发展的水平限制,我们不能事先预计每项治疗对于每一个患者都有效。一旦初始治疗失败或不能够耐受初始治疗,就需要进行二线治疗替代,这种治疗被称为抢救性治疗(salvage therapy)。
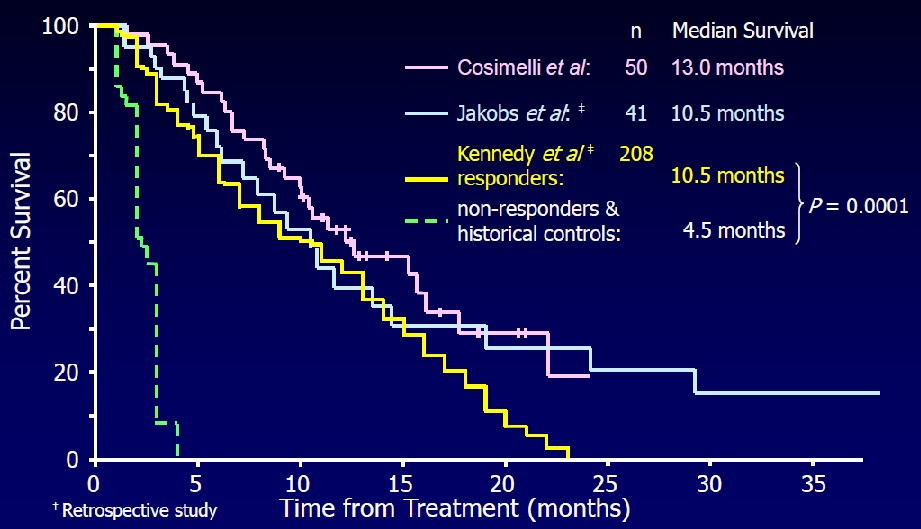
SIR-Spheresin salvage therapy of mCRC: Comparison of Overall Survival【12,13,15】
Cosimelli M et al. Br J Cancer 2010; 103: 324–331.; Jakobs T et al. JVIR 2008; 19: 1187 ;Kennedy A et al. Int J Radiat Oncol Biol Phys2006; 65: 412–25. SIR-Spheresin “Salvage Therapy” of Chemo-RefractorymCRC
Hendlisz et al. J Clin Oncol 2010;28:3687–94. Phase III Trial Comparing Protracted Intravenous Fluorouracil Infusion Alone or With Yttrium-90 Resin Microspheres Radioembolization for Liver-Limited Metastatic Colorectal Cancer Refractory to Standard Chemotherapy
Radioembolization with 90Y-resin microspheres plus FU is well tolerated and significantly improves TTLP and TTP compared with FU alone. This procedure is a valid therapeutic option for chemotherapy-refractory liver-limited mCRC. 结论:TTLP 和TTP 90Y > FU Rühl J et al. Eur J Cancer Suppl2009;7:343 Abs. 6071. Cosimelli et al. Br J Cancer 2010;103:324–31. (没找到文献) Jakobs et al. J Vasc Interv Radiol2008;19:1187–95.Cianni et al. Cardiovasc Interv Radiol 2009;32:1179–86. Cianni et al. Cardiovasc Interv Radiol 2009;32:1179–86.
Nace et al. Int J Surg Oncol 2011; ePub.
Kennedy A et al. Int J Radiat Oncol Biol Phys2006; 65: 412–25.
SIR-Spheresin 2nd-line Treatment of mCRC
1. Bipat S, van Leeuwen MS, Ijzermans JN, Comans EF, Planting AS, Bossuyt PM, Greve JW, Stoker J. Evidence-base guideline on management of colorectal liver metastases in the Netherlands. Neth J Med. 2007 Jan;65(1):5-14. Review. 2. Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007 Mar;18(3):581-92. Epub 2007 Feb 7. 3. McMillan DC, McArdle CS. Epidemiology of colorectal liver metastases. Surg Oncol. 2007 Jul;16(1):3-5. Epub 2007 May 9. 4. Manfredi S , Lepage C, Hatem C, Coatmeur O, Faivre J, Bouvier AM Epidemiology and management of liver metastases from colorectal cancer. Ann Surg. 2006 Aug;244(2):254-9. 5. Poston GJ. Surgical strategies for colorectal liver metastases. Surg Oncol. 2004 Aug-Nov;13(2-3):125-36. 6. Khatri VP, Chee KG, Petrelli NJ. Modern multimodality approach to hepatic colorectal metastases: solutions and controversies. Surg Oncol. 2007 Jul;16(1):71-83. Epub 2007 May 29. http://www.ncbi.nlm.nih.gov/pubmed/18358928 7. Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, Bechstein WO, Primrose JN, Walpole ET, Finch-Jones M, Jaeck D, Mirza D, Parks RW, Collette L, Praet M, Bethe U, Van Cutsem E, Scheithauer W, Gruenberger T. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC intergroup trial 40983): a randomised controlled trial. Lancet. 2008;371:1007–1016. 8. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S, Holmgren E, Ferrara N, Fyfe G, Rogers B, Ross R, Kabbinavar F. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–2342 9. Falcone A, Ricci S, Brunetti I, Pfanner E, Allegrini G, Barbara C, Crinò L, Benedetti G, Evangelista W, Fanchini L, Cortesi E, Picone V,Vitello S, Chiara S, Granetto C, Porcile G, Fioretto L, Orlandini C, Andreuccetti M, Masi G; Gruppo Oncologico Nord Ovest. Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: the Gruppo Oncologico Nord Ovest. J Clin Oncol. 2007 May 1;25(13):1670-6. 10. Gray B, Van Hazel G, Hope M, Burton M, Moroz P, Anderson J, Gebski V. Randomised trial of SIR-Spheres plus chemotherapy vs. chemotherapy alone for treating patients with liver metastases from primary large bowel cancer. Ann Oncol. 2001;12:1711–1720. 11. Van den Eynde M, Flamen P, El Nakadi I, Liberale G, Delatte P, Larsimont D, Hendlisz A. Inducing resectability of chemotherapy refractory colorectal liver metastasis by radioembolization with yttrium-90 microspheres. Clin Nucl Med. 2008;33:697–699 12. Kennedy AS, Coldwell D, Nutting C, Murthy R, Wertman DE, Jr, Loehr SP, Overton C, Meranze S, Niedzwiecki J, Sailer S. Resin 90Y-microsphere brachytherapy for unresectable colorectal liver metastases: modern USA experience. Int J Radiat Oncol Biol Phys. 2006;65:412–425. 13. Jakobs TF, Hoffmann RT, Dehm K, Trumm C, Stemmler HJ, Tatsch K, La Fougere C, Murthy R, Helmberger TK, Reiser MF. Hepatic yttrium-90 radioembolization of chemotherapy-refractory colorectal cancer liver metastases. J Vasc Interv Radiol. 2008;19:1187–1195. 14.Kennedy AS, Nutting C, Coldwell D, Gaiser J, Drachenberg C. Pathologic response and microdosimetry of (90)Y microspheres in man: review of four explanted whole livers Int J Radiat Oncol Biol Phys. 2004 Dec 1;60(5):1552-63. 15.Cosimelli M, Golfieri R, Cagol PP, Carpanese L, Sciuto R, Maini CL, Mancini R, Sperduti I, Pizzi G, Diodoro MG, Perrone M, Giampalma E, Angelelli B, Fiore F, Lastoria S, Bacchetti S, Gasperini D, Geatti O, Izzo F; Italian Society of Locoregional Therapies in Oncology (SITILO). Multi-centre phase II clinical trial of yttrium-90 resin microspheres alone in unresectable, chemotherapy refractory colorectal liver metastases Br J Cancer. 2010 Jul 27;103(3):324-31. doi: 10.1038/sj.bjc.6605770. Epub 2010 Jul 13. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||